As a Master of Design candidate at University of Cincinnati, I have been studying contraceptive decision-making. This interest sprung from reading about the alarmingly high teen pregnancy and HIV/AIDS rates in my immediate environment in Cincinnati as well as nationally in the US. What’s further alarming is the diversity in the population affected by this. It is no longer a low-income or low-education crisis. Women like myself are making irrational decisions and compromising their own agency, which I believe is the only method of 100% self-protection. Several design opportunities lie in creating engaging digital content, de-stigmatizing communication through tools & educational information systems among others.
Clinical data records have shown that certain populations are receiving disproportionate access to reproductive healthcare. Teen pregnancy affects all racial/ethnic groups, but African-American and Latina teens share a disproportionate burden (Galloway, Duffy, Dixon, Fuller, 2016). This disparity is often a consequence of economic conditions, social structures and disparate access to resources. While a lot of scholarly work is being directed towards the unique needs of at-risk populations, there is relatively less focus on the perceptions towards contraception itself, which may be a determinant in decision-making.

Ohio has no model curriculum for sex education, leaving decisions up to local education committees assembled for this planning. The adapted curricula falls into three categories: abstinence-centered (or abstinence- only until marriage), abstinence-plus and comprehensive. However, the mandatory stress on Abstinence, is continually disregarded by students. In 2015, 42.4% of never-married female teenagers (4.0 million) and 44.2% of never-married male teenagers (4.4 million) had had sexual intercourse at least once by the end of high-school (Abma, Martinez 2017).
Through this thesis, I seek to bridge the gaps between the regulatory formal sex education taught at schools, by leveraging informal channels of sex education that the students are already engaged in. These would include improving parent-child communication, active roles for healthcare providers and also online dissemination of scientifically accurate information. Several design opportunities lie in creating engaging digital content, de-stigmatizing communication through tools & educational information systems among others.
Ongoing Literature Review
Over the course of the last 15 weeks I have conducted convergent and divergent secondary research on the subject, based on the initial findings of gendered and racial disparity. The following sections illustrate the several factors that influence contraceptive decision-making and their role in doing so.
2.1 Disparities in sexual health
Disparities in teen pregnancy and birth rates are driven in part by differential access to contraception and reproductive health care services, as well as a host of complex social determinants (Dehlendorf, Rodriguez, Levy, et al. 2010). Research has also found that African-American and Latina youth are less likely to have insurance and to access routine primary health care services. (Woodruff, Zimmerli, Duncan, 2006)
The far-reaching consequences of such varied racial, social and structural contributors to the nonuse of contraception is resulting in high and disproportionate rates of unwanted teen pregnancies, the spread of STIs, single-parent households with economic insecurity and the societal stigma that it draws. In America, among non-Hispanic white teens, the birth rate in 2015 was 19 births per 1,000, while among African-American teens, it was 39 births per 1,000. Latina teens have the highest birth rate, at 42 births per 1,000 teens according to the National Campaign to Prevent Teen Pregnancy (NCPTP).
2.2 Current state of sex education in Ohio
Ohio does not have a sex education curriculum, but it does have guidelines for each district to build their own curriculum based on their communities needs. Even with the given guidelines, designing a sex education curriculum can be a challenging task, considering each local school district is left to prioritize subject matter based on time and their own resources. Adding to these differences in content, schools also have the autonomy to decide at what age to teach a certain topic. In Ohio, many schools do not start teaching sex education until high school, but some start exploring the human body and sexuality in third grade (Gregory, Dennis, and Tucker, 2015). So the advancement in topics and when they are taught is determined by where the child goes to school.
2.3 Political contentions and religiosity

Sex Education or contraception in Ohio cannot be exclusively discussed without addressing politics and religiosity. The ‘Fetal Heartbeat Bill’ was passed in April 2019, making Ohio the sixth state to ban abortion as early as six weeks into pregnancy. The right-to-life movement in Ohio primarily Catholic and pivots on the belief that all life is sacred, beginning at conception, as stated in article 5 of the Fifth Amendment ‘You shall not kill: and whoever kills shall be liable to judgment.’ In 1973, the Roe V. Wade decision liberalised abortion in all fifty states. As a result, the abortion issue effectively transformed the US political landscape and continued to cause unrest.
2.4 Underlying Social Structures
Quantitative data suggests that African-American women are likely to be in racially homogenous partnerships resulting in continues poor economic conditions. (Norwood and Zhang, 2015). This is supported by the lingering effects of Redlining in the United States, that continue to situate like-with- like limiting early exposure to other races. Taking, for example, Georgia, in Macon today, 91 per cent of redlined neighbourhoods are inhabited by mostly minorities; 73 per cent of such neighbourhoods remain low-to- moderate income (Jan T, 2018, Washington Post).
Another social structure affecting sexual health among African-American is the disproportionate prevalence of African-American men in U.S. prisons coupled with the much higher STI rate among previously incarcerated Black men (as much as 10 times higher than the general population) (Behforouz & Chang, 2010). This severely disturbs the sex ratio, leaving less free men for more women, resulting in higher infidelity. This fails the perceived efficacy of the contraceptive measures these women might have taken. This theory posits that health behaviors, such as condom use, are determined by individuals’ knowledge of health risk, or agency to control. (Norwood, Zhang, 2015)
2.5 Predicted sexual recession
Earlier this year, the Centers for Disease Control and Prevention reported a decline in the share of high school students who said they ever had sex: from 47 per cent in 2005 to 41 per cent in 2015. Gen Y and Gen Z are more cautious on average than earlier generations, and hence more inclined to focus on the emotional and physical risks of sex, rather than its joys. Some of these factors include unprecedented exposure to negative health outcomes due to commercialization and broadcasting. Movements like ‘Me Too’ have also unintendedly caused growing concerns about what borders unwanted or assaultive sex. (Wilcox and Sturgeon, 2018)
Trend forecasters are speculating how the surge in smartphone ownership seems to coincide with the marked, recent declines in sex among young adults and teenagers. The evidence is growing that the spread of highly entertaining and diverting technology discourages in-person socializing, including one of the most fundamental forms of socializing: sex. (DePaulo, 2018) .
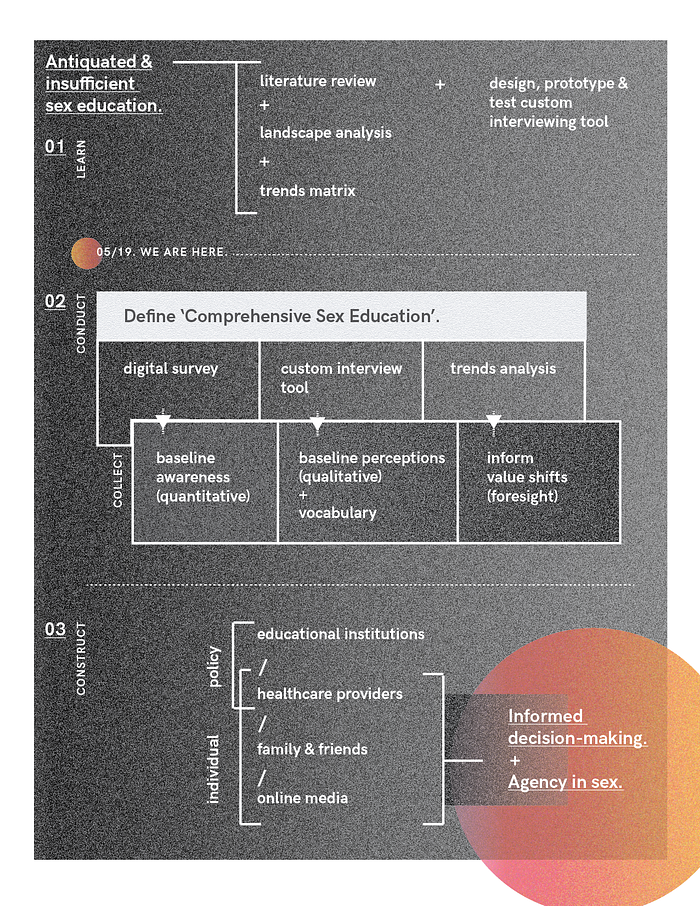
Design Methodology

Having conducted the literature review to expand on my interest, I designed a custom interviewing tool in Translational Research course.

The tool enables candid conversation on sensitive topics like mine, with three outputs: vocabulary around the subject, qualitative perceptions and a baseline awareness of the participants. Using this tool to conduct a well-rounded discussion on the subject, I will develop baseline personas of adolescents, parents and health workers, to be able to target their nuanced barriers.
These insights along with an ongoing trend analysis will inform the trend forecast, where I want to substantiate and illustrate a future that can be altered by my intervention(s). This would require both the vision of a dystopic future, to show how and at what touchpoints do my solutions play a role and also a utopic future, assuming my solutions get implemented to their full capacity.
A large part of the work will be towards making, releasing and testing prototypes of multifaceted solutions directed at:
- engaging and empowering adolescents
- supporting and educating parents
- de-stigmatizing teen healthcare access
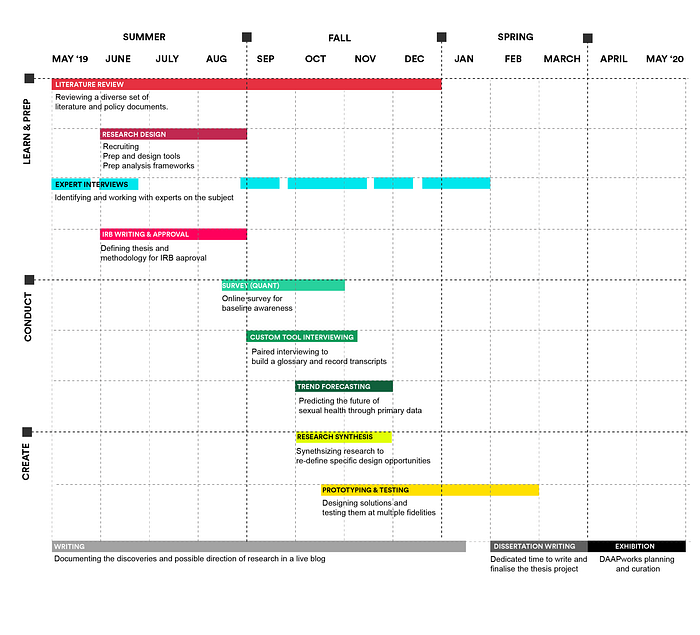
Nerdy timeline for the coming semesters